Knowledge
What’s Your WHY? Mobility For The Neurotype
Neurotyping, Rehab, mobility & injury prevention, Strength and performance

What's Your WHY? Mobility For The Neurotype
Mobility. mo·bil·i·ty. mōˈbilədē. It’s a hot topic of late. It’s also a topic of debate: “Increase your mobility, but not too much. Too much mobility sacrifices stability”. This article is not about picking sides around this debate, but rather about catching it from another angle.
Mobilization – What’s Your WHY?
I was lucky to attend a conference recently where I heard Jean-François Ménard speak. J-F is a re-known sports psychologist, founder and president of Kambio Performance, a company specialized in elite mental performance services. Among others, he works with Tessa Virtue and Scott Moir, but even more importantly, he is a fantastic speaker. He spoke to us about remembering your WHY as a way to guide HOW you will get to your goal and WHAT you will do to get there, and his presentation really stuck with me.
All interventions that target the human body need to be adjusted to context. Mobility is defined as: the ability to move or be moved freely and easily. To move or to be moved is the context. Essentially, it’s your WHY. For most of us, our WHY is to move. We want to improve mobility to move better, have better range of motion, squat lower, run faster, etc. “To be moved” is what we tend to see as passive mobility or flexibility, and “the debate” says that passive mobility is “useless” for all kinds of reasons you have heard that I will not reiterate here. What I will do however, is look at this from another angle and dig deeper into finding the WHY.
In the Movement Optimization Course, the Mobilization sequence is part of a comprehensive strategy that directs various assessment and corrective tools towards an intervention for moving better. The objective of the Mobilization sequence is to “create space”, which serves to:
• Improve joint positioning
• Improve movement appreciation (improved perception of the capacity to move)
• Downregulate/inhibit facilitated/hypertonic muscles or compensatory movement patterns
To create space becomes the WHY we use mobility. HOW you create space and WHAT tools you will use to do it is 100% about the client. Movement is behavior-based and people move in ways that are influenced by their perception of what they can and cannot do. You need to work with their perception to determine whether they will need “to move” or “to be moved” to most efficiently create space.
When I assess a client’s range of motion, I bucket them into one of two categories based their perception of their own limitation, that is, what they feel is preventing them from moving into the full range of motion. I use the following two buckets:
A “mechanical” perception of limitation means that the client’s perception is that they cannot stretch the muscle enough (or that the muscle is too tight) to move into the full ROM.
A “neural” perception of limitation means that the client’s perception is that a “strength” or control problem is preventing them from moving into the full ROM.
For all intents and purposes, “mechanical” and “neural” are in quotations as I am not proposing that a mechanical perception of limitation has no neural contribution and vice versa. Rather, I am suggesting that people who give “mechanical” answers like: “It feels really tight here” or “It really pulls here” will create space differently than people who give “neural” answers like: “I can’t get there without turning/arching/etc.” or “I can’t get the contraction I need to get there”. You could use whatever bucket titles you like, what’s important is gaining insight on the client’s perception of limitation, which you will then use to determine HOW you will help them create space. A mechanical mobilization strategy must allow the client to feel the tight structures being stretched, as that is their subjective perception of limitation. A neural mobilization strategy must help the client move into the ROM, as their subjective perception of limitation is the feeling that they cannot get into the required position.
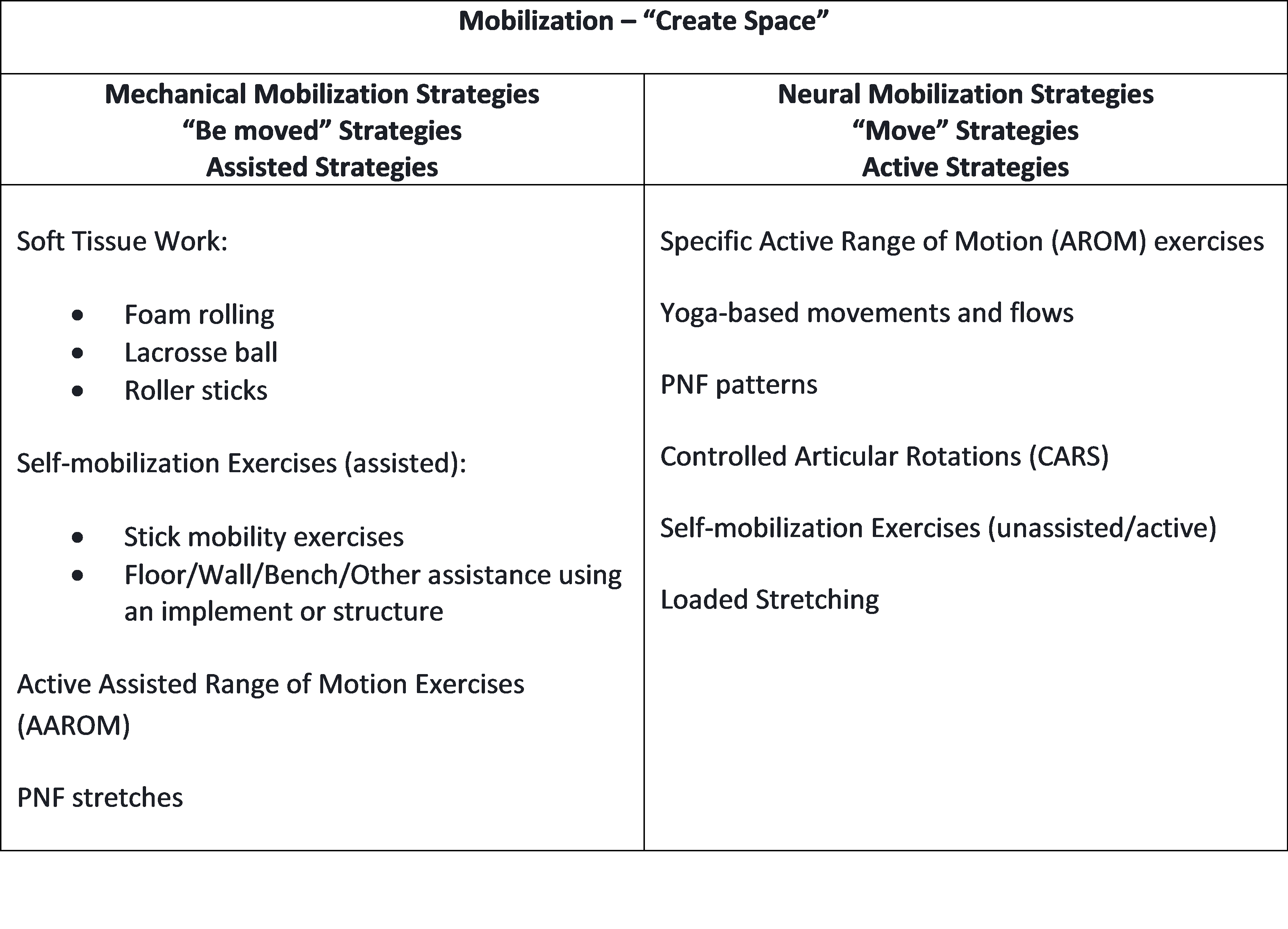
If we think back to our definition of mobility, the mechanical type typically needs to be moved to create space, while the neural type typically needs to move. So, what was initially our WHY we work on mobility now becomes our HOW we will work on it. The table below provides examples of what strategies would be mechanical vs neural. Interchangeably, these categories could be “Be Moved” Strategies and “Move Strategies”, or “Assisted Strategies” and “Movement Strategies. Of course, this process of categorizing client perceptions is not empirically validated. It is only meant to be a guideline, what is most important is that you remember the WHY. Have you successfully created space? If you have not, you will need to try a different strategy or maybe simply a different tool within the strategy. For example, a mechanical strategy might work quite well with a neural type to help them “move into” the position.
Here is an example of an assisted self-mobilization exercise for the T-spine:
Here is an example of a specific active ROM exercise for the hip:
Applying a Mobilization Strategy To The Neurotype
If you are certified in Neurological and Physical Typing, you can take this strategy even further, by adjusting your Mobilization strategy based on the Neurotype. For ease of writing, I will simply refer to individuals who have a mechanical perception of limitation as mechanical, and the same for neural.
Type 1
Type 1 is intense (1A) and explosive (1B). They are a neurodominant profile, which means that to feel good, they must have high nervous system involvement. Please do not confuse this with the neural perception of limitation bucket or assume that all Type 1 will have a neural perception. In fact, I have worked with many who were quite mechanical. What you do need to remember when prescribing mobilization exercises for Type 1 is that they need to be challenged, they need to feel they are doing something. So, if you have a mechanical Type 1, soft tissue work will likely not be your best strategy. It’s too parasympathetic and passive for them (again, this is not ALWAYS true, remember that what’s important is going back to your WHY). You might want to opt for higher tension exercises like PNF stretching and AAROM. If you have a neural Type 1, loaded stretching is the best option, as it really presents a challenge for them, plus they love and are accustomed to whole-body tension kind of work. For more on loaded stretching: https://thibarmy.com/loaded-stretching-one-powerful-versatile-training-method/
Here’s an example of an active-assisted ROM exercise for the hip:
Type 2
Type 2 like a faster training pace, so organizing your mobilization exercises into a circuit is a good idea. The Type 2A are all about variety, so you could use whichever tool within the strategy that they fit into, mechanical or neural, but you will need to change it up frequently. This is challenge because if you really want to create change, frequency of practice is key. Therefore, change up the exercises and approaches, but make sure you keep mobilizing the same target regions. Type 2B is all about sensation and love the mind-muscle connection, so PNF stretches work quite well with a mechanical type. Soft tissue work could work as well, but not too much or for too long. A neural Type 2B will fare well with CARS and unassisted self-mobilization exercises because of the mind-muscle connection component and the slower tempo.
Here is an example of CARS for the shoulder:
Here is an example of an unassisted self-mobilization exercise for the T-spine:
Type 3
Type 3 is about precision and control. They are high stress, so parasympathetic strategies like soft-tissue work are great for them. With a Type 3, opt for a strategy that is simple. Something too complex will create stress for them and/or, they will overanalyze and not get the benefit of creating space. For example, a neural Type 3 might really like the control and precision of CARS, just make sure they are not overly segmenting it. On the other hand, PNF patterns are likely not your best option, because they involve segmenting the rotation and flexion/extension component and Type 3 will likely over-think it.
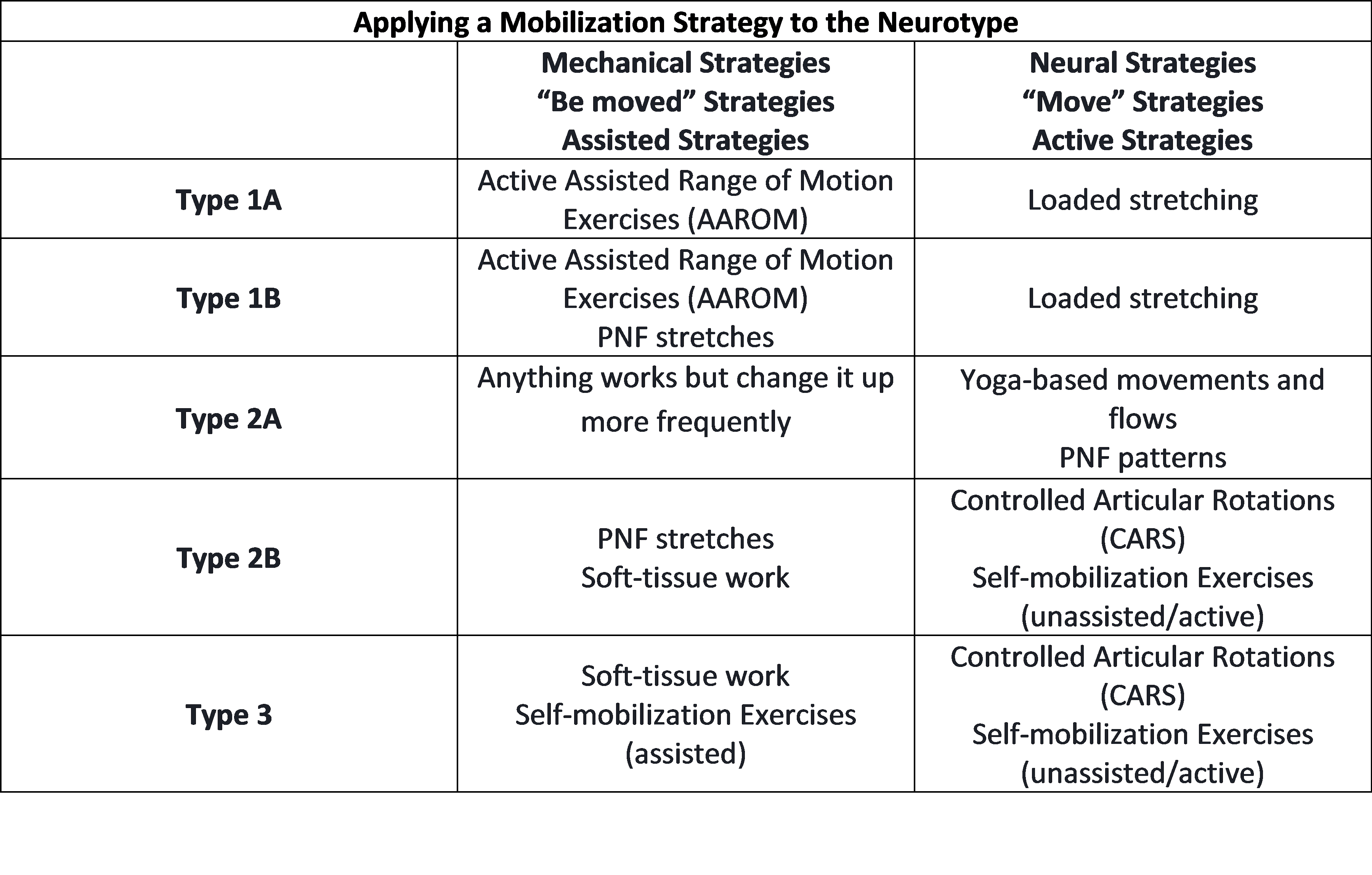
Here’s a quick reference chart by Neurotype. I want to reiterate that the most important thing is remembering the WHY. Don’t reduce this to thinking that only certain categories work for specific Neurotypes, that is not the intent of this chart, nor this article.
 At the beginning of this article, I included a quote: “There is no right or wrong, there is only cause and effect”. We’re too quick to categorize something as right or wrong, to dismiss something as useless and promote something else as useful. Foam rolling is not bad. Heck, even passive stretching is not all bad if it helps create space. What’s important is to follow-up and make a connection with that space. In the Movement Optimization Course, that’s the role of the Activation and Integration sequences, and the sum of Mobilization, Activation and Integration is what promotes mobility AND stability.
At the beginning of this article, I included a quote: “There is no right or wrong, there is only cause and effect”. We’re too quick to categorize something as right or wrong, to dismiss something as useless and promote something else as useful. Foam rolling is not bad. Heck, even passive stretching is not all bad if it helps create space. What’s important is to follow-up and make a connection with that space. In the Movement Optimization Course, that’s the role of the Activation and Integration sequences, and the sum of Mobilization, Activation and Integration is what promotes mobility AND stability.
So, if you’re foam rolling and lacrosse balling day in and day out with everyone, it’s not wrong, you just need to question whether it is optimal depending on who you’re working with. It may simply need to be paired with something else to make it more effective and contribute to a complete and individualized workout prep. Remember the WHY.
-MLD